In oral mucosa, radiation effects appear early in the course of therapy. The severity of the local tissue reactions depends on the radiation dose, the size of each radiation fraction, the volume of tissue irradiated, the fractionation scheme, and the type of ionizing radiation used. Recent research efforts have shed some light on the pathophysiology of these acute and late changes. This program describes the changes, and the efforts that have bee made in recent years to minimize the acute effects (radiation mucositis). In addition the program discusses the recent significant rise in radiation trismus observed in patients undergoing chemoRT and the comments on the effect of dynamic bite openers used for prevention.
Maxillofacial Prosthetics – Radiation Effects Mucosa, Taste, Jaw Opening — Course Transcript
- 1. 3. Radiation Effects – Mucosa, Taste, Jaw Opening John Beumer III, DDS, MS Eric Sung, DDS Division of Advanced Prosthodontics, Biomaterials and Hospital Dentistry and UCLA School of Dentistry All rights reserved. This program of instruction is covered by copyright ©. No part of this program of instruction may be reproduced, recorded, or transmitted, by any means, electronic, digital, photographic, mechanical, etc., or by any information storage or retrieval system, without prior permission of the authors.
- 2. Radiation Effects – Mucosa, Taste, Jaw Opening Treatment and Preventionv Mucosa v Acute effects v Mucositis v Fungal infections v Management of mucositis v Taste apparatus v Late effects v Mucous membranes v Muscle v Skin v Edemav Jaw opening v Dynamic bite openers
- 3. Radiation Effects – Oral Mucous MembranesEarly changes in oral mucous membranes v Pathophysiology of oral mucositis (Sonis, 1998, 2004)
- 4. Pathophysiology- Radiation MucositisSonis model (1998, 2004) Initiation l Reactive oxygen species results in breaks in DNA strands Primary damage response l NF-kB l Upregulation of genes producing proinflammatory cytokines Signal amplification l Colonization of oral bacteria leads to production of additional cytokines which lead to more tissue damage Ulceration Healing
- 5. Radiation Mucositis Key – FactsPresents initially as an erythematous reaction which soondevelops into oral ulcerations covered with pseudomembranes.Severity dependent upon:v Clinical treatment volume, dose and fractionation.v Sites: The less keratinized the mucosa the more severe the mucosal reactionsv More severe in patients presenting with chronic alcoholism and liver cirrhosisv More severe in patients with insulin dependent diabetesv Severity may be lessened by a reduction of oral bacterial loadsMucositis is more severe in patients.receiving concomitant chemotherapy.
- 6. Radiation Mucositis – Key Facts v It is one of the most clinically significant side effects of treatment. v Its frequency and severity limit the aggressiveness of therapy and may interrupt or preclude completion of therapy. v It has a significant impact on the cost of care (Peterson et al, 2001). v There is no effective treatment. v Palliation of symptoms is the only possible approach at present..
- 7. Radiation Mucositis – Key Facts v Incidence – 80% per cent or more depending upon the dose per fraction (Vinssink et al, 2003) v Secondary to radiation induced mitotic death of the cells composing the basal layer of the epithelium (Scully and Epstein, 1996; Dumbrique et al, 2000). v Rarely seen when the dose per fraction is below 180 cGy per fraction (Silverman, 2003).
- 8. MucositisOral mucositis begins as an erythematous reaction associatedwith the tumor site generally after about 7-10 days of thetherapy. This erythema is accompanied by soreness and aburning sensation.
- 9. Mucositisv The erythematous reaction is followed by ulceration. With conservativetreatment approaches the ulcerations remain confined to the tissues associatedwith the tumor volume.v With more aggressive treatment (ie. Chemoradiation) the mucositis is moreextensive involving normal tissues adjacent to the gross tumor volume.v With conservative treatment approaches the mucosa re-epithelializes 2-4weeks following completion of therapy. If concomitant chemotherapy is employed, twice or longer the usual time is required for re-epithelization.
- 10. MucositisIn most patients the ulcerations remains confined to the tumorsite. After radiation the ulcerations re-epithelialize and becomecovered with “normal” appearing oral mucosa. However, if concomitant chemotherapy is employed these ulcerations may take several months to heal.
- 11. MucositisBackscatter – Mucositis is particularly localized in thispatient. This results when a metallic crown rests against oralmucous membrane and is in the path of the radiation beam.Prevention is easily accomplished by displacing the buccalmucosa or tongue away from the crown with a stent.
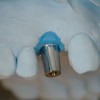
- 12. BackscatterTitanium reconstruction plates, implants, traysand mesh (Schwartz et al, 1979; Mian et al, 1987) Dose enhancement at the bone implant interface is about 15-18%.
- 13. Backscatter Irradiation of existing implantsBackscatter- This patient received 6000 cGy postoperatively.Previously, a fibula free flap had been used to reconstruct amandibular continuity defect. Implants were placed at thesame time the fibula was placed.
- 14. Backscatter Irradiation of existing implantsFollowing radiation, the patient developed a dehiscence over theleft implant which eventually lead to exposure of bone. The two leftimplants were eventually lost. A piece of bone was sequestratedand eventually this area became covered with mucosa.
- 15. BackscatterIrradiation of existing implantsHowever, the flap was not lost andmandibular continuity was maintained.
- 16. Acute Effects – Oral Mucous Membranes Patients with compromised oral mucous membranes secondary to chronic alcoholism with liver cirrhosis or insulin dependent diabetes and those treated with chemoradiation may develop more severe mucositis. A BIn patient “A” virtually all of the epithelium on the soft palate waslost and therapy had to be interrupted to allow the mucosa to re-epithelialize. In patient “B” the tongue became depapillated buttherapy was completed without interruption.
- 17. Acute Effects – Oral Mucous Membranes Candida albicans infectionDuring the administration of radiation therapy acute candidiasis can occur(Ramirez-Amador, etal, 1997).Topical therapy: It is best managed by nystatin suppositories used as an orallozenge (100,000 units per suppository) or by the use of nystatin oral rinse(100,000 units per cc). If the patient is wearing dentures, they should besoaked in a nystatin solution daily. If the patient has difficulty dissolving the lozenges intraorally because of xerostomia, a nystatin oral suspension is a useful alternative.
- 18. Acute Effects – Oral Mucous Membranes Candida albicans infectionSystemic therapy: *Prolonged use of antifungalv Ketoconazole (200 mg daily agents is discouraged with food) because of the risk ofv Fluorconozole ( 100 mg daily) developing fungal resistance. (Silverman, 2003) Systemic therapy is preferred in the potentially noncompliant patient.
- 19. Acute Effects – Oral Mucous Membranesv Changes in the oral flora during therapy are thoughtto intensify radiation mucositis (Ramirez-Amador etal, 1997).v Colonization by gram negative bacilli (Spijkervet,1991) appear to induce more severe mucosalreactions such as the reaction in this patient.
- 20. Acute Effects – Oral Mucous MembranesManagement of mucositis during therapy v At present there is no effective approved means of reducing the severity of oral mucositis v During the past 15 years 1his field has been the subject of intense study
- 21. TreatmentManagement of mucositis during therapy Continues to be supportive and symptomatic v Saline and soda rinses v Viscous xylocaine v Systemic analgesics v Antifungal medications
- 22. Treatment of Mucositis Research Approachesv Radioprotective agentsv Anti-inflammatory agentsv Mucosal decontaminationv Growth factors
- 23. Treatment of Mucositis Research ApproachesRadioprotective agents – Free radical andreactive oxygen inhibitorsv Amifostinev Benzydaminev N-acetylcysteine
- 24. Treatment of Mucositis Research Approaches Radioprotective agents – Free radical and reactive oxygen inhibitors (Antonadou et al, 2002; Buntzel et al, 2002; Sonis, 2004; Law et al, 2007) v Amifostine v Benzydamine v N-acetylcysteine” These agents act as free radical and ROS scavengers and theoretically minimize much of the deleterious effects of irradiation on normal cells.” These drugs are also potent anti-inflammatory agents.
- 25. Treatment of Mucositis Research Approaches Radioprotective agents – Free radical and reactive oxygen inhibitors (Antonadou et al, 2002; Buntzel et al, 2002; Sonis, 2004; Law et al, 2007 v Amifostine v Benzydamine v N-acetylcysteine” The data is has been contradictory and study designs have been questioned (Sutherland and Bowman, 2001).” Concern voiced regarding tumor uptake and impact on tumor response (Vissink et al, 2003).
- 26. Treatment of Mucositis Research ApproachesMucosal decontamination v Chlorhexidine – Has not shown to be effective in reducing the severity of mucositis (Spijkervet et al, 1989; Epstein et al, 1992; Foote et al, 1994; Dodd et al, 1996; Adamietz et al, 1998). v Antibacterial lozenges targeting gram negative bacillus (combination of amphotericin B, polymyxin, and tobramycin) have shown some promise in reducing the severity of mucositis (Spijkervet et al, 1990, 1991; Symonds et al, 1996; Wijers et al, 2001; Mellroy, 2007)
- 27. Treatment of Mucositis Research ApproachesGrowth factors l Keratin growth factor (KGF) l Granulocyte-macrophage stimulating factor May promote more rapid healing by stimulating surviving stem cells but have the potential of affecting the tumor response
- 28. Chemoradiationv Used as an adjunct or concomitantlyv Oral side effects are more severe • Acute effects § Oral mucositis is more severe and generally takes 3 to 8 months to resolve as opposed to the 2-4 weeks when radiation alone is given. Some patients are unable to complete therapy because of the side effects. § About one half of the patients need “G” tubes placed in order to make it through radiation.
- 29. . Chemoradiation Late effects v Incidence of scarring and fibrosis, osteoradionecrosis and soft tissue necrosis appears much higher when used in conjunction with CRT. Little data available when used with IMRT v Asubstantial number of patients are unable to swallow after therapy secondary to atrophy and fibrosis associated with the muscles of the pharynx. These patients must be fitted with permanent “G” tubes. v Increasing number of patients suffer from velopharyngeal incompetence, velopharyngeal sufficiency and trismus after chemoradiation secondary to fibrosis and atrophy of the muscles associated with mastication and velopharyngeal function.
- 30. Acute Effects – Taste Apparatusv Taste acuity is readily affected by tumoricidal doses of radiation (Sandow et al, 2006; Mirza et al, 2008).v Dramatically effects the quality of life (Redda and Allis, 2006v Changes in taste cells and buds are due to both the direct and indirect effects of irradiation (Yamashita et al, 2006).
- 31. Acute Effects – Taste Apparatusv Architecture of the taste buds is almost completely eliminated at 5000 cGy.v Alterations in taste acuity are first noticed during the second week of therapy (Conger and Wells, 1969; Conger, 1973; Silverman et al, 1983).v Perception of bitter and acid flavors is more susceptible to impairment than salt and sweet
- 32. Acute Effects – Taste Apparatusv Taste generally returns to “near normal” 2-4 following re- epithelialization if salivary flow is reasonable.v In patients with severe xerostomia following radiation the number of buds is decreased, their morphology is altered and taste may not return to normal.v Reduction may also be secondary to loss of nerve fibers innervating the taste budsv Clinical trials with Zinc supplements have shown promise (Silverman et al, 1983; Ripamonte et al, 1998; Matsuo et al, 2000)
- 33. Acute Effects – Olfactionv Since the olfactory epithelium is high in the nasal passage and often not within the clinical treatment volume smell is less affectedv Smell thresholds after radiation exposure are increased dramatically (Ophir et al, 1988).v Few if any patients experience complete recovery
- 34. Late Effects – Oral Mucous Membranesv Scarring and fibrosis of lamina propriav Telangiectasia – dilation and coalescence of small venules close to the surface of the epitheliumv Epithelial layer is thinner and less keratinized Clinical significance: The oral mucosa is easily traumatized or perforated. The ulcerations that develop are slow to heal because of the reduced vascularity and fibrosis of the underlying connective tissue.Clinical significance: The denture bearing mucosal surfaces arecompromised making tolerance of complete dentures difficult.
- 35. Late Effects – Oral Mucous Membranes Scarring and telangiectasia In most patients scarring and telangiectasia are confined to the tumor site ( arrow).
- 36. Late Effects – Oral Mucous Membranes Scarring and telangiectasiaWhen the telangiectasias extend beyond the localtumor volume as in these two patients, it indicates:v The patient tolerated the radiation poorly.v The dose to the normal adjacent tissues was brought to the highest level of tissue tolerance.v The patient was treated with concomitant chemoradiation
- 37. Late effects Muscle wasting and fibrosisv In patients treated for pharyngeal, soft palate and base oftongue tumors, fibrosis and muscle wasting of the muscles ofpharyngeal wall and the soft palate responsible forvelopharyngeal closure leads to velopharyngeal insufficiency.v These changes are more common in patients treated withchemo-radiation and many patient are unable to swallow aftercompletion of radiation therapy.
- 38. Late effects Muscle wasting and fibrosisThis patient was treated with external beam plus brachytherapyfor a squamous carcinoma of the tongue. The volume of tissueencompassed by the implant was larger than normal because oftumor size and infiltration. The tumor dose exceeded 8500 cGy ina large volume of the tongue.
- 39. Late effects Muscle wasting and fibrosisAfter completion of therapy the tongue mass was reducedand tongue mobility and control impaired. Speech articulationwas dramatically affected and salivary control compromised.
- 40. Late Effects – Oral Mucous MembranesThis patient received 6800 cGy external beam therapy (CRT) fora squamous cell carcinoma of the anterior floor of the mouth.Note the scarring at the tumor site (arrow). However, there areno signs of radiation effects beyond the tumor site.This patient would be a good candidate for complete dentures. She iscompliant and the scarring and telangiectasia is confined to the tumor site.However, overextension of the lingual flange in this region could result in amucosal perforation and lead to an osteoradionecrosis.
- 41. Late Effects – Oral Mucous Membranes Patient received 6800 cGy for a squamous cell carcinoma of the anterior floor of the mouth. Note the telangiectasias within the zone of keratinized attached mucosa (ovals)This patient would be a poor candidate fora lower complete denture because thebearing surface mucosa is thin andatrophic and could be easily perforated bya complete denture.
- 42. Late Effects – Oral Mucous MembranesPatient received 6800 cGy for a squamous cell carcinoma ofthe anterior floor of the mouth. Note the telangiectasias withinthe zone of keratinized attached mucosa (ovals)However, a maxillary complete denture would predispose to little risk.These patients learn to masticate by mashing the bolus against the rugaepattern, incorporated within the denture, with the tongue.
- 43. Soft Tissue Necrosis A mucosal ulcer in irradiated tissue that has no residual tumorClinical signs: The first priority is to rule outa) Extremely painful recurrent tumor.b) No inflammatory halo Diagnostic methods used:c) No induration Cytology, biopsy and clinical observation
- 44. Late Effects – Oral Mucous Membranes” Soft Tissue Necrosis – Patient received 5500 cGy via external beam and another 2500 cGy with a radium implant for a squamous cell carcinoma of the lateral border of the tongue.” Nine months after therapy he developed this ulceration at the site of the tumor.” Cytology and biopsy were negative and a diagnosis of radiation soft tissue necrosis was assumed.” The lesion epithelialized 4 months later
- 45. Acute Effects – Skin ReactionsIn most patients skin reactions are limited toerythema and tanning of the skin.Individuals with light complexions are likely to have the most severe skin reactions.
- 46. Acute Effects – Skin Some patients develop dry and moist desquamation of the skin.
- 47. Late Effects – Skin Scarring and telangiectasiaThis patient received 5600 cGy for a squamous carcinomaof the right cheek. After therapy he developed scarring andtelangiectasia of the cheek skin.
- 48. Late Effects – Skin Alopecia, and hyper-pigmentationNote the hair loss within the radiation field. This finding can bevery useful in identifying the fields of radiation when examininga male post radiation (if CRT was used) particularly when theradiation records are not available. Note the hyperpigmentation(oval).
- 49. Late effects – Edemav Secondary to obliteration of small lymphatic channels and worsened by scarring and fibrosis (Engerset, 1964; Sherman and O’Brien, 1967).v Clinically significant when it effects the tongue and buccal mucosav Generally most prominent in the submental and submandibular areasv Radical neck dissection potentiates the effects and increases the edema
- 50. Edema Both patients present with edema of oral cavity structures, one involving the tongue, the other the buccal mucosa. These two patients are susceptible to tongue and cheek biting.Prevention: Accomplished by use of a prosthetic stent designed to displacethe buccal mucosa or tongue away from the interocclusal surfacesIn edentulous patients the enlargement of the tongue has negative effects onthe floor of the mouth contour and adversely affects the lingual extension andthe patients ability to tolerate and control the lower denture.
- 51. Radiation and Trismusv Secondary to fibrosis of the muscles of mastication and generally not noticed until 3-6 months after radiation (Goldstein et al, 1999)v The higher the dose the greater the trismus (Goldstein et al, 1999).v Occurrence is 10-45% (Kent et al, 2008).v Mouth opening following radiation is reduced by 18% (Dijkstra, 2004)v The rate and severity is much higher in patients treated with chemoRTv Occurs more often when radiation is combined with a surgical procedure (i.e. radical maxillectomy) that effects the TMJ and the muscles of mastication.v Risk and severity increases with time particularly in patients treated with chemoRTv IMRT may decrease the risk (Hsiung et al, 2008)
- 52. Radiation and Trismusv Dramatically worsened by concomitant chemotherapyv Maximum opening may be reduced to 5-15 mmv Treatment consists of exercise and use of dynamic bite openers (Dijkstra et al, 2004).v Progressively worsens with time.v Compromises the use of complete dentures, obturator prostheses.*In patients with combined radiation and surgery, early initiation of an exerciseprogram before the fibrosis sets in provides the best results.
- 53. Radiation and Trismusv This represents maximum opening for this patientv 13 years ago patient was treated with chemoRT for a nasopharyngeal carcinoma
- 54. Radiation Trismus -Treatmentv Dynamic bite openers*# are the most effective form of treatment (Dijkstra, 2004)v Patient is instructed to stretch with the device for 30 minute sessions three times per day.v Requires a high level of patient cooperation because of the discomfort associated with the required manipulationv Tongue blades, taped together and used as a lever have been less effective in increasing mouth opening. *Therabite Corp., West Chester, PA #Dynasplint Systems Inc., Severna Park, MD
- 55. v Visitffofr.org for hundreds of additional lectures on Complete Dentures, Implant Dentistry, Removable Partial Dentures, Esthetic Dentistry and Maxillofacial Prosthetics.v The lectures are free.v Our objective is to create the best and most comprehensive online programs of instruction in Prosthodontics
- 56. Referencesl Scully C and Epstein J. (1996) Oral health care for the cancer patient. Oral Oncol Eur J Cancer 32:281-92.l Dumbrigue H, Sandow P, Nguyen K, et al. (2000) Salivary epidermal growth factor levels decrease in patients receiving radiation therapy to the head and neck. Oral Surg Oral Med Oral Path Oral Radiol Endod 89:710-16.l Silverman S. (2003) Complications of treatment. in Oral Cancer 5th edition ed S. Silverman BC Decker Inc. Hamilton, London pp 113-128.l Vissink A, Jansma F, Spijkervet F et al. (2003) Oral sequellae of head and neck radiotherapy. Crit Rev Oral Biol Med 14:199-.l Vissink A, Burlage F, Spijkervet J, et al. (2003) Prevention and treatment of the consequences of head and neck radiotherapy. Crit Rev Oral Biol Med 14:213-225l Sonis S. (2004) Oral mucositis in cancer therapy. J Support Oncol 2:3-8.l Sonis S. (1998) Mucositis as a biological process: A new hyposthesis for the development of chemotherapy induced stomatotoxicity. Oral Oncol 34:39-43.l Denham J, Peters L, Johansen J, et al. (1999) Do acute mucosal reactions lead to consequential late reactions in patients with head and neck cancer? Radiother Oncol 52:157-164.
- 57. Referencesl Spijkervet F, van Saene H, van Saene J, et al. (1990) Mucositis prevention by selective elimination of oral flora in irradiated head and neck cancer patients. J Oral Pathol Med 19:486-9.l Spijkervet F, van Saene H, van Saene J, et al. (1991) Effect of selective elimination of the oral flora on mucositis in irradiated head and neck patients. J Surg Oncol 46:167.l Spijkervet, F, van Saene H, Panders A, et al. (1989) Effect of chlorhexidine rinsing on the oropharyngeal ecology in patients with head and neck cancer patients. Oral Surg Oral Med Oral Path 67:154-161.l Martin M. (1993) Irradiation mucositis: a reappraisal. Oral Oncol Eur J Cancer 2:81.l Ramirez-Amador V, Silverman S, Mayer P, et al. (1997) Candidal colonization and oral cnadidiasis in patient undergoing pharyngeal radiation therapy. Oral Surg Oral Med Oral Path Oral Radiol Endod 84:149-153.l Peterman A, Cella D, Glandon G et al. (2001) Mucositis in head and neck cancer: economic and quality of life outcomes. J Natl Cancer Inst Monogr 29:45-51.l Antonadou D, Pepelassi M, Synodinou M et al. (2002) Prophylactic use of amifostine to prevent radiochemotherapy induced mucositis and xerostomia in head and neck cancer. Int J Radiat Oncol Phys 52:739-47
- 58. Referencesl Bunzel J, Glatzel M, Kuttner K et al. (2002) Amifostine in simultaneous radio- chemotherapy of advanced head and neck cancer. Semin Radiat Oncol 12:4-13l Law A, Kennedy T, Pellitteri D, et al. (2007) Efficacy and safety of subcutaneous amisfostine in minimizing radiation induced toxicities in patients receiving combined modality treatment for squamous cell carcinoma of the head and neck. Int J Radiat Oncol Biol Physics. 69:1361-68.l Sutherland S, Browman G. (2001) Prophylaxsis of oral mucositis in irradiated head cancer patients : a proposed classification scheme of interventions and meta-analysis of randomized-clinical trials. Int J Radiat Oncol Biol Phys 49:917-30.l Makkonen TA, Minn G, Jekunen et al (2000) Granulocyte macrophage-colony stimulating factor (GM-CSF) and sucralfate in prevention of radiation induced mucositis. A prospectifve randomized study. In J Radiat Oncol Biol Phys 46:525-534.l Epstein J, Vickers L, Spinelli J, et al. (1992) Efficacy of chlorhexidine and nystatin rrinses in prevention of oral complications in leukemia and bone marrow transplantation. Oral Surg Oral Med Oral Path 73:682-689.l Foote R, Loprinzi C, Frank A, et al. (1994) Randomized trial of a chlorhexidine mouthwash for alleviation of radiation-induced mucositis. J Clin Oncol 12:2630-33.a
- 59. Referencesl Dodd M, Larson P, Dibble S, et al. (1996) Randomized clinical trial of chlorhexidine versus placebo for prevention of oral mucositis in patient receiving chemotherapy. Oncol Nurs Forum 23:921-7.l Adamietz I, Hahn R, Bottcher H et al. (1998) Prophylaxe der radiochemootherapeutishch bedingten mucositis. Strahlenther Onkol 174:149-55.l Symonds R, McIlroy P, Khorrami P, et al. (1996) The reduction of radiation mucositis by selective decontamination antibiotic pastilles: A placebo controlled double blind trial. Br J Cancer 74:312-17l Wijers O, Levendag P, Harms E, et al. (2001) Mucositis reduction by selective elimination of oral flora in irradiated cancers of the head and neck: A placebo controlled double blind randomized study. Int J Radiat Oncol Biol Phys 50:343-52.l Mc Ilroy P. (2007) Radiation mucositis: A new approach to prevention and treatment. Eur J Cancer Care 5:153-58.l El-Sayed S, Epstein J, Minish E, et al. (2002) A pilot study evaluating the safety and microbiologic efficacy of an economically viable antimicrobial lozenge in patients with head and neck cancer receiving radiation therapy. Head and Neck 24:6-15.
- 60. Referencesl Beumer J, Curtis T, Harrison R. (1979a) Radiation therapy of the oral cavity: Sequellae and management. Part I. Head Neck Surg 1:301-12.l Cooper J, Fu K, Marks J, Silverman S. (1995) Late effects of radiation therapy in the head and neck region. Int J Radiat Oncol Biol Phys 31:1141-64l Dion M, Hussey D, Osborn J. (1990) Preliminary results of a pilot study of pentoxifylline in treatment of late radiation soft tissue necrosis. Int J Radiat Biol Phys 19:401-7.l Ruo, Redds MG, Allis S. (2006) Radiotherapy – induced taste impediment. Cancer 32:541-7l Sandow P, Hejrat-Yazdi, Heft M. (2006) Taste loss and recovery following radiation therapy. J Dent Res 85:608-11.l Mirza N, Machtay M, Devine P, etal. (2008) Gustatory impairment in patient undergoing head and neck irradiation. Laryngoscope 118:24-31.l Conger A. (1973) Loss and recovery of taste acuity in patients irradiated to the oral cavity. Radiat Res 53:338-47.l Conger A. (1969) Radiation and aging effect on taste structure and function. Radiat Res 37:31-49.l Silverman JE, Weber CS, Silverman S Jr. (1983) Zinc supplementation and taste in head and neck cancer patient undergoing radiation therapy. J Oral Med 38:14-16.
- 61. Referencesl Yamshita H, Nakagawa K, Tago M, et al. (2006) Taste dysfunction in patients receiving radiotherapy. Head and Neck 28:508-16.l Matsuo R. 2000. Role of saliva in the maintenance of taste sensitivity. Crit Rev Oral Biol Med 11:216-29.l Henkin R, Talal N, Larson A, et al. (1972) Abnormalities of taste and smell in Sjorgren’s syndrome. Ann Int Med 76:375-83.l Ripamonte C, Zecca E, Brunelli C, et al. (1998) A randomized controlled clinical trial to evaluate the effects of zinc sulfate on cancer patients with taste alterations caused by head and neck irradiation. Cancer 82:1938-45.l Ophir, D., Gitterman, A., Gross-Isseroff, R. (1988) Changes in smell acuity induced by radiation exposure of the olfactory mucosa. Arch Otolaryngol Head Neck Surg 114:853-55.l Engerset A. (1964) Irradiation of lymph nodes and vessels; experiments in rats with reference to cancer therapy. Acta Radiol. 229(supp):5-125l Sherman JO, O’Brien PH. (1967) Effects of ionizing radiation on normal lymphatic vessels and lymph nodes. Cancer 20:1851-8l Dijkstra P, Kalk W, Roodenburg J. (2004) Trismus in head and neck oncology: A systematic review. Oral Oncol 40:879-89.
- 62. Referencesl Goldstein M, Maxymiw WG, Cummings BJ et al. (1999) The effects of antitumor irradiation on mandibular opening and mobility: A prospective study of 58 patients. Oral Surg Oral Med Oral Path Oral Radiol Endod 88:365-73l Kent L, Brennan M, Noll J, et al. (2008) Radiation induced trismus in head and neck cancer patients. Support Care Cancer 16:305-9.l Hsiung C-Y, Huang E-Y, Ting H-M, et al. (2008) Intensity-modulated radiotherapy for nasopharyngeal carcinoma: The reduction of radiation-induced trismus. Brit J Radiol 81:809-14.l Driezen S, Brown L, Handler S, et al. (1976) Radiation induced xerostomia in cancer patients – effect on salivary and serum electrolytes. Cancer 38:273.l Driezen S, Daly T, Drane J. (1977) Prevention of xerostomia-related dental caries in irradiated cancer patients. J Dent Res 56:99-104.l Brown L, Driezen S, Rider L, et al. (1976) The effect of radiation- induced xerostomia on salivary lysozyme and immunoglobulin levels. 0ral Surg Oral Med Oral Path 41:83-92.l Marks J, Davis C, Gottsman V et al. (1981) The effects of radiation on parotid salivary function. Int J Radiat Oncol Biol Phys 7:1013-19.l Sodicoff M, Pratt N Shollely M. (1974) Ultrastructural radiation injury of rat parotid gland. Radiat Res 58:196-208.
- 63. Referencesl Paardekooper G, Cammelli S, Zeilstra L, et al. (1998) Radiation apoptosis in relation to acute impairment of rat salivary gland function. Int J Radiat Biol 73:641-48.l Coppes R, Zeilstra L, Kampinga H, et al. (2001) Early to late sparing of radiation damage to the parotid gland by adrenergic and muscarinic receptor agonists. Brit J Cancer 85:1055-63.l Coppes R, Roffel A, Liekele J, et al. (2000) Early radiation effects on muscarnic receptor-induced secretory responsiveness of the parotid gland in the freely moving rat. Radiat Res 153:339-46.l Konings AW, Coppes RP, Vissink A. On the mechanism of salivary gland radiosensitivity. Int J Radiat Oncol Biol Phys 62:1187-94.l Shannon, I., Suddick, R. (1976) Saliva. in Dental Biochemistry ed Lazzari, E Lea and Febiger, Philadelphia pp 201-242.l Curtis T, Griffith M, Firtell D. (1976) Complete denture prosthodontics for the radiation patient. J Prosthet Dent 36:66-76.l Marunick M, Seyedsadr M, Ahmad K, et al. (1991) The effect of head and neck cancer treatment on whole salivary flow. J Surg Oncol 48:81-6.l Eisbruch A, Randall K, Haken T, et al. (1999) Dose, volume and function relationship in parotid salivary glands following conformal and intensity modulated irradiation of head and neck cancer. Int J Radiat Oncol Biol Phys 45:577-87.
- 64. Referencesl Eisbruch A, Rhodus N, Rosenthal N, et al. (2003) How should we measure and report radiotherapy-induced xerostomia? Sem Radiat Onc 13:226-34.l Franzen L, Fungegard U, Ericson T, et al. (1992) Parotid gland function during and following radiotherapy of malignancies in the head and neck. Eur J Cancer 28:457-62.l Roesink J, Moerland M, Battermann J et al. (2001) Quantitative dose-volume response analysis of changes to parotid gland function after radiotherapy in the head and neck region. Int J Radiat Oncol Biol Phys 51:938-46.l Eisbruch A, Kim H, Terrell J, et al. (2001) Xerostomia and its predictors following parotid-sparing irradiation of head and cancer. Int J Radiat Oncol Biol Phys 50:695-704.l Konings A, Faber H, Cotteleer F, et al. (2005) Secondary radiation damage as the main cause for unexpected volume effects: A histopathologic study of the parotid gland. Int J Radiat Oncol Biol Physics. 64:98-105.l Mira J, Fullerton G. Wescott W. (1981) Some factors influencing salivary function when treating with radiotherapy. Int J Radiat Oncol Biol Phys 71:535-41.l Makkonen T, Tenovuo J, Vilja P et al. (1986) Changes in the protein composition of whole saliva during radiotherapy in patients with oral or pharyngeal cancer. Oral Surg Oral Med Oral Path Oral 62:270-75.
- 65. Referencesl Valdez J, Atkinson J, Ship J, et al. (1993) Major salivary gland function in patients with radiation-induced xerostomia: Flow rates and sialochemistry. Int J Radiat Oncol Biol Phys 25:41-7l Almstahl A, Wikstrom M, Groenink J. (2001) Lactoferrin, amylase and mucin MUC5B and their relation to oral microflora in hyposalivation of different origins. Oral Microbiol Immunol 16:345-52.l Driezen S, Brown L, Handler S, et al. (1976) Radiation induced xerostomia in cancer patients – effect on salivary and serum electrolytes. Cancer 38:273-8.l Anderson MW, Izutsu KT, Rice JC. (1981) Parotid pathophysiology following mixed gamma and neutron irradiation of cancer. Oral Surg Oral Med Oral Pathol 52:495-500.l Fox P, Vander Van P, Baum B, et al. (1986) Pilocarpine for the treatment of xerostomia associated with salivary gland dysfunction. Oral Surg Oral Med Oral Pathol 61:243-8.l Greenspan D, Daniels T. (1989) The effectiveness of pilocarpine in post radiation xerostomia. Cancer 59:1123-5.l Johnson J, Ferretti G, Nethery J, et al. 1993. Oral Pilocarpine for post- irradiation xerostomia in patients with head and neck cancer. New England J. Med 329:390-5.
- 66. Referencesl Rieke J, Haferman M, Johnson J, et al. (1995) Oral pilocarpine for radiation- induced xerostomia: Integrated efficacy and safety results from two prospective randomized clinical trials. Int J Radiat Oncol Biol Phys 31:661-9.l Niedermeier W, Matthaeus C Meyer et al. (1998) Radiation induced hyposalivation and its treatment with oral pilocarpine. Oral Surg Oral Med Oral Path 44:541-9l Shannon I, McCary B, Starcke E. (1977) A saliva substitute for use by xerostomic patients undergoing radiotherapy to the head and neck. Oral Surg Oral Med Oral Path 44:656-61.l Shannon I, Wescott W, Starke E et al. (1978a) Laboratory study of colbalt 60 irradiated human dental enamel. J Oral Med 33:23-7.l Visch LL, Gravenlmade EJ, Schaub EN et al. (1986) A double blind crossover trial of CMC and mucin containing saliva substitutes. Int J Oral Maxillofac Surg 15:395-400.l Roesink J, Konings A, Terhaard H et al. (1999) Preservation of the rat parotid function after radiation by prophylactic pilocarpine treatment: Radiation dose dependency and compensatory mechanisms. . Int J Radiat Oncol Biol Phys 45:483-9.l Warde P, O’Sullivan B, Aslanidis J, et al. (2002) A phase III placebo- controlled trial of oral pilocarpine in patients undergoing radiotherapy for head and neck cancer. Int J Radiat Oncol Biol Phys 54:9-13.
- 67. Referencesl Burlage F, Roesink J, Kampinga H, et al. (2008) Protection of salivary function by concomitant pilocarpine during radiotherapy: A double blind, randomized, placebo-controlled study. Int J Radiation Onc Biol Phys 70:14-22.l Lombaert I, Wierenga P, Kok T, et al. (2006) Mobilization of bone marrow stem cells by granulocyte colony-stimulating factor ameliorates radiation-induced damage to salivary glands. Clin Cancer Res 12:1804-12.l Lombaert I, Brunsting J, Wierenga P, et al. (2008a) Rescue of salivary gland function after stem cell transplantation in irradiated glands. Plosone.org vol 3 issue 4 e2063.l Lombaert I, Brunsting J, Wierenga P et al. (2008b) Cytokine treatment improves parechymal and vascular damage of salivary glands after irradiation. Clin Cancer Res 14:7741-50.l Lombaert I, Brunsting J, Wierenga, P et al. (2008c) Keratinocyte growth factor prevents radiation damage to salivary glands by expansion of the stem/ progenitor pool. Stem Cells 26:2595.l Delanian S, Lefaix J. (2004) The radiation-induced fibroatrophic process: Therapeutic perspective via the antioxidant pathway. Radiother Oncol 73:119-131.l Lyons A and Ghazali N. (2008) Osteoradionecrosis of the jaws: Current understanding of its pathophysiology and treatment. Brit J Oral Maxillofac Surg 46:65360.
- 68. Referencesl Rohrer M, Kim Y, Fayos J. (1979) The effect of cobalt-60 irradiation on monkey mandibles. Oral Med Oral Surg Oral Path 48:424-40.l Van Merkesteyn J, Bakker D, Borgmeijer-Hoelen A. (1993) Pathogenesis and treatment of osteoradionecrosis of the jaws. Abstracts Int Acad for Oral Onc #3l Silverman S, Chierici G. (1965) Radiation therapy of oral carcinoma – I. Effects on oral tissues and management of the periodontium. J Periodont 36:478-84.l Fugita M, Tanimoto K, Wada T. (1986) Early radiographic changes in radiation bone injury. Oral Surg Oral Med Oral Path 61:641-44.l Epstein J, Lunn R, Le N, Stevenson-Moore P. (1998) Periodontal attachment loss in patients after head and neck radiation therapy. Oral Surg Oral Med Oral Path Oral Radiol Endod 86:673-77.l Beumer J, Harrison R, Sanders B, et al. (1984) Osteoradionecrosis: predisposing factors and outcome of therapy. Head and Neck Surg 6:819-27.l Yusof Z and Bakri M. (1993) Severe progressive periodontal destruction due to radiation tissue injury. J Periodontol 64:1253-58.l Castanera T, Jones D, Kimeldorf D. (1963) Gross dental lesions in the rat induced by x-rays and neutrons. Radiat Res 20:577-85.
- 69. Referencesl Walker R. (1975) Direct effects of radiation on the solubility of human enamel in vitro. J Dent Res 54:901.l Wiemann MR, Davis MK, Besic FC (1972) Effects of x-radiation on enamel solubility of human teeth in vitro. J Dent Res 51:868l Shannon I, Trodahl J, Starke E. (1978b) Remineralization of enamel by a saliva substitute designed for use in irradiated patients. Cancer 41:1746-50.l Jansma J, Borggreven J, Driessens F, et al. (1990) Effect of x-ray irradiation on the permeability of bovine dental enamel. Caries Res 24:164-8.l Kielbassa A, Beetz I, Schendera A, et al. (1997) Irradiation effects on the microhardness of fluoridated and non-fluoridated dentin. Eur J Oral Sci 105:444-7.l Kielbassa A, Hinkelbein W, Hellwig, E et al. (2006) Radiation damage to dentition. Lancet Onc 7:326-35.l Gowgiel JM. (1960) Experimental radio-osteonecrosis of the jaws. J Dent Res 39:176-97.l Collett, W.R., Thonard, J.C. (1965) The effect of fractional radiation on dentinogenesis in the rat. J Dent Res 44:84-90.
- 70. Referencesl Koppang H. (1967) Studies on the radiosensitivity of the rat incisor. Odont Tidskr 75:413-50l Fawzi M, Shklar G, Krakow A. (1985) The effect of radiation on the response of the dental pulp to operative and endodontics procedures. Oral Surg Oral Med Oral Path 59:405-13.l Toljanic J, Saunders V. (1984) Radiation therapy and management of the irradiated patient. J Prosthet Dent 52:852-8.l Gorlin R, Meskin L. (1963) Severe irradiation during odontogenesis. Oral Surg 16:35-8.l Pietrokovski J, Menczel J. (1966) Tooth dwarfism and root under development following irradiation. Oral Surg 22:95-9.l Dahllof G, Rozell B, Forsberg C, et al. (1994) Histologic changes in dental morphology induced by high dose chemotherapy and total body irradiation. Oral Surg Oral Med Oral Path Oral Radiol Endod 77:56-60.l Kaste S, Hopkins K, Jenkins J. (1994) Abnormal odontogenesis in children treated with radiation and chemotherapy. Am J Roentgenol 162:1407-11.l Llory H, Damron A, Frank R. (1971) Changes in the oral flora following buccal pharyngeal radiotherapy. Arch Oral Biol 16:617-30.l Llory H, Damron A, Gionanni M, et al. (1972) Some population changes in oral anaerobic microorganisms, streptococcus mutans, and yeast following irradiation of salivary glands. Caries Res 6:298-311.
- 71. Referencesl Brown R, Driezen S, Handler S, et al. (1975) The effect of radiation induced xerostomia on human oral microflora. J Dent Res 54:740-50.l Keene H, Daly T, Brown L, et al. (1981) Dental caries and streptococcus mutans prevalence in cancer patients with irradiation-induced xerostomia 1-13 years after radiotherapy. Caries Res 15:416-27.l Keene H and Flemming T. (1987) Prevalence of caries associated microflora after radiotherapy in patients with cancer of the head and neck. Oral Surg Oral Med Oral Path 64:421-6.l Epstein J, McBride B, Stevenson-Moore P, et al. (1991) The efficacy of chlorihexidine gel in reduction of Streptococcus mutans and Lactobacilus species in patients treated with radiation therapy. Oral Surg Oral Med Oral Path 71:172-8.l Weerkamp A, Wagner K, Vissink A, et al. (1987) Effect of the application of mucin-based saliva substitute on the oral microflora of xerostomic patients. J Oral Pathol 16:474-8.l Freymiller EG, Sung EC, Friedlander AH. (2000) Detection of radiation- induced cervical atheromas by panoramic radiograph. Oral Oncol 36:175-9.l Zidar N, Ferluga D, Hvala A, et al. (1997) Contribution to the pathogenesis of radiation-induced injury to large arteries. J Laryngol Otol 111:988-90.
- 72. Referencesl Eisele DW, Koch DG, Tarazi AE, Jones B. (1991) Aspiration from delayed radiation fibrosis of the neck. Dysphagia. 6:120-22.l Kang MY, Holland JM, Stevens KR Jr. (2000) Cranial neuropathy following curative chemotherapy and radiotherapy for carcinoma of the nasopharynx. J Laryngol Otol 114:308-10.l Sharabi Y, Dendi R, Holmes C, Goldstein D. (2003) Baroreflex failure as a late sequela of neck irradiation. Hypertension. 42:110-116.l Hardman PD, Tweeddale PM, Kerr GR, et al. (1994) The effect of pulmonary function of local and loco-regional irradiation for breast cancer. Radiother Oncol 30:33-42.l Basavaraju SR, Easterly CE. (2002) Pathophysiological effects of radiation on atherosclerosis development and progression, and the incidence of cardiovascular complications. Med Phys 29:2391-2403.l Stewart JR, Fajardo LF, Gillette SM, et al. (1995) Radiation injury to the heart. Int J Radiat Oncol Biol Phys 31:1205-11.l Gyenes G, Rutqvist LE, Liedberg A, Fornander T. (1998) Long term cardiac morbidity and mortality in a randomized trial of pre- and postoperative irradiation therapy versus surgery along in primary breast cancer. Radiother Oncol 48:185-90.
- 73. Referencesl Khan MH, Ettinger SM. (2001) Post mediastinal radiation coronary artery disease and its effect on arterial conduits. Catheter Cardiovasc Interv 52:242-8.l Hall E. (2000) Radiobiology for the radiobiologist. Philadelphia: Lippincott, Williams and Wilkens.
- 74. The EndClick to return to main
New Lectures
 Cement Retention vs Screw Retention
Cement Retention vs Screw Retention
John Beumer III DDS, MS
Robert Faulkner DDS, MS
Robert Faulkner DDS, MS
 Single Tooth Defects in Posterior Quadrants
Single Tooth Defects in Posterior Quadrants
John Beumer III DDS, MS
Robert Faulkner, DDS
Robert Faulkner, DDS
 Restoration of Posterior Quadrants and Treatment Planning
Restoration of Posterior Quadrants and Treatment Planning
John Beumer III DDS, MS
Robert Faulkner, DDS
Kumar C. Shah DDS, MS
Robert Faulkner, DDS
Kumar C. Shah DDS, MS
 Angled Implants
Angled Implants
John Beumer III DDS, MS
Allesandro Pozzi, DDS
Allesandro Pozzi, DDS