Esthetic display of retainers is a concern of most patients. This program instruction discusses the methods used to idealize the esthetic result of patients fitted with removable partial dentures. Topics include clasp selection and position, attachments and their proper use, and rotational path RPD’s.
Removable Partial Dentures – Esthetics – Rotational Path and Attachments — Course Transcript
- 1. Esthetics, Use of Attachments and Rotational Path RPD’s John Beumer III DDS, MS Division of Advanced Prosthodontics UCLA School of Dentistry and Eugene King DDS Section of Dental Oncology MD Anderson Hospital and Tumor InstituteThis program of instruction is protected by copyright ©. No portion of thisprogram of instruction may be reproduced, recorded or transferred by anymeans electronic, digital, photographic, mechanical etc., or by anyinformation storage or retrieval system, without prior permission.
- 2. Esthetics, Use of Attachments and rotational path RPD’s
- 3. “I” bar vs circumferential clasp Circumferential clasp on the cuspid
- 4. Esthetics“I” bars vs circumferential
- 5. Esthetics v Low smile line v Cuspid –lateral splinted v Occlusion v Anterior guidance v Posterior – Lingualized with centric only contact
- 6. Esthetics – I” bars5 year post delivery followup. vNote low smile line vWidened major connector vPositive cingulum rests vOcclusion vAnterior guidance using the cuspids vLingualized posterior occlusion with centric only contact
- 7. Esthetics
- 8. Esthetics – “I” Barsv Extension Base RPD opposing implant supported fixed hybrid prosthesisv Occlusion v Anterior guidance with the anterior teeth v Posterior occlusion-lingualized with centric only contact
- 9. RPD AttachmentsAdvantages: v Elimination of visible clasp armsDisadvantages: v Additional expense v Increased frequency of adjustment and failure v Increased technical expertise required v Unpredictable or unfavorable distribution of forces
- 10. Attachment ClassificationRigid attachments v No movement is possible between the parts. Used in situations where the abutment teeth fully support the occlusal forces (tooth borne RPD’s and fixed partial dentures)Resilient attachments v Allows movement to take place between the parts, thus providing stress-breaking. An example is the ERA attachment
- 11. Attachments – Resilient ERA attachment – Extra-coronal resilient attachmentThe ERAattachmentpermits the RPDto be displacedinto theedentulousextension areaby up to .4 mm
- 12. Attachments – ResilientERA attachment – Extra-coronal resilient attachmentPlastic burnout pattern Metal housing ERA attachment
- 13. Attachments – ResilientERA attachment – Extra-coronal resilient attachment Requirements for use vSplinted abutments vRest distant from the attachment vClose followup to consider relines ERA Attachment
- 14. Attachments – Resilient ERA attachment – Extra-coronal resilient attachment ERA ERA + splintingPhotoelastic analysis – Evaluating the following: vSplintedvs unsplinted vRest vs no rest vRest positionBerg and Caputo et al
- 15. Attachments – Resilient ERA attachment – Extra-coronal resilient attachment ERA ERA+splintingSummary and conclusions vAttachment best used when: v Adjacent teeth splinted v Positive rests v Light retention (white and orange attachment)
- 16. Attachments – ResilientERA attachment – Extra-coronal resilient attachment v Splinting the abutments helps distribute the forces v Positive rests away from the extension area helps direct the forces vertically onto the abutment and into the edentulous bearing surfaces v Less wear of ERA attachment
- 17. Overlay denture attachmentsAdvantages v Improved esthetics v Maintain support v More favorable biomechanics – Improved crown- root ratio
- 18. Overlay denture attachmentsProblems v Copings become loose v Attachment wear, loss & breakage v Alveolar resorption v Overdenture breakage v Pt. maintenance problems v Pt. oral hygiene problems
- 19. Attachments – Resilient ERA attachment – Extra-coronal resilient attachment This patient is status post partial palatectomy for a benign tumor of theleft hard palate. The left tuberosity remains and it contains a third molar
- 20. Use the surveyor to prepare the path of insertion for the attachments
- 21. Use the surveyor to prepare the path of insertion for the attachments
- 22. Attachments – Resilient ERA attachment – Extra-coronal resilient attachmentNote the bracing arm through the proximal of #5 and #6. It isnon- retentive but keeps the RPD framework from beingdisplaced lingually in this region and with the cingulum rest on#8, keeps the framework centered over the ERA attachment. Bracing arm Rest ERA attachment Cingulum rest
- 23. Attachments – Resilient ERA attachment – Extra-coronal resilient attachment Bracing armThe two central incisors havebeen splinted together. Acingulum rest is positioned onthe mesial side of #8. The ERA High smileattachment is incorporatedwithin the crown of #9. Note the bracing arm.
- 24. Attachments – Resilient ERA attachment – Extra-coronal resilient attachment High smileNote the attachment associated with third molar. This serves as an occlusalstop and has a retentive attachment incorporated within. The ERA should notbe used unless a positive occlusal stop is present on the defect side,either from a tooth or an implant.
- 25. Attachments – ResilientERA attachment – Extra-coronal resilient attachment Occlusion v Right side – Anterior guidance v Left side – Mutually protected occlusion
- 26. Magnetic AttachmentsAdvantages : v Ease of insertion and removal v Simple laboratory work & economic cost v Reduced lateral forces v No leverage v No fragile parts for fracture v No activation necessary v Do not need special equipment (parallelometer etc) v Easy to maintain oral hygiene
- 27. Magnetic AttachmentsApplications v Retained roots v Implants v Maxillofacial Prosthetic Applications
- 28. Magnetic AttachmentsMaxillofacial applications
- 29. Magnetic AttachmentsMaxillofacial applications
- 30. Magnetic AttachmentsMaxillofacial applications
- 31. Magnetic Attachments Maxillofacial applications
- 32. Inappropriate use of attachmentsv Insufficient vertical movement allowedv Cantilever forces delivered to the abutmentsv Result v High rate of periodontal breakdown and abutment tooth fracture
- 33. Inappropriate use of attachmentsv Cantilever forces delivered to the abutmentsv Result v High rate of periodontal breakdown and fracture of the abutment teeth
- 34. Inappropriate use of attachmentsNonresilient Attachments in Extension Based RPD’s v No vertical movement permitted v Cantilever forces delivered to the abutments v Result v High rate of periodontal breakdown and fracture
- 35. Inappropriate use of attachmentsNonresilient Attachments in Extension Based RPD’sv No vertical movement permittedv Cantilever forces delivered to the abutmentsv Result v High rate of periodontal breakdown and fracture of the abutment teeth
- 36. Inappropriate use of attachments Nonresilient Attachments in Extension Based RPD’sv No vertical movement permittedv Cantilever forces delivered to the abutmentsv Result v High rate of periodontal breakdown and fracture of the abutment teeth
- 37. Kennedy Class IV RPD’sRotational Path of Insertion RPD’s
- 38. Rotational Path of Insertion RPD’sv One portion is inserted first permitting rigid portions of the RPD (proximal plates) to engage undercutsv The prosthesis is then rotated into positionv In the posterior quadrants limited to tooth borne RPD’sv Most often used to restore anterior extension defects where use of attachments or clasps is unfavorable
- 39. Rotational Path of Insertion RPD’sAdvantage v Elimination of unesthetic retainers (clasp arms) v The clasp arms are replaced by rigid retainers v These rigid retainers engage undercuts and consist of a positive rest and a minor connector (proximal plate)
- 40. Rotational Path of Insertion RPD’sCaution v Little tolerance for error. It requires a high level of sophistication on the part of both the dentist and the lab technician v Requires well prepared positive rests seats. May require restorations to develop an acceptable rest seat v Undercuts in posterior rest seats will prevent proper seating
- 41. Rotational Path of Insertion RPD’sv They can also be used to restore Kennedy Class III RPD’s with missing posterior teethv Disadvantage v Bracing from guide planes is compromised
- 42. Rotational Path of Insertion RPD’sTreatment planning v Patientpresents with moderate periodontal bone loss with recent loss of the incisors v Options v Fixed partial denture v Implant supported fixed partial denture v Rotational path of insertion RPD
- 43. Rotational Path of Insertion RPD’sTreatment planning v Patientpresents with moderate periodontal bone loss with recent loss of the incisors v Options v Fixed partial denture – Problems v Length of span v Amount of tooth reduction for PFM’s v Long pontics – Compromised esthetic result
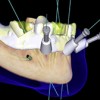
- 44. Rotational Path of Insertion RPD’sTreatment planning v Patient presents with moderate periodontal bone loss with recent loss of the incisors v Options v Implant supported fixed partial denture – Problems v Difficult to predictably restore vertical and horizontal boney contours with grafting
- 45. Rotational Path of Insertion RPD’sTreatment planning v Patientpresents with moderate periodontal bone loss with recent loss of the incisors v Options v Rotational path of insertion RPD -Best solution v Minimal reduction of tooth structure v Best esthetic result v Least costly
- 46. Rotational Path of Insertion RPD’s Tentative RPD design
- 47. Rotational Path of Insertion RPD’sSurveying the cast v Identify the cast orientation that results in at least a . 25 mm undercut on each of the anterior abutments
- 48. Rotational Path of Insertion RPD’sSurveying the cast v Tilt cast to determine initial path of insertion.
- 49. Rotational Path of Insertion RPD’sSurveying the cast v Verify that at this cast inclination, proper rests can be developed consistent with the initial path of insertion. v The rests must not be undercut in relation to the path of insertion
- 50. Rotational Path of Insertion RPD’sv Prepare the anterior and posterior rests. v The rests must be positivev Beware of excessive buccal inclination of the maxillary molars. The rests must be positive but should not be undercut in relation to the path of insertion
- 51. Rotational Path of Insertion RPD’sv Fabricatethe RPD casting and verify the adaptation
- 52. Rotational Path of Insertion RPD’sCompleted RPD Important factors for long term success v Positive rests v Survey for appropriate undercuts and proper rotational path of insertion
- 53. Rotational Path of Insertion RPD’sv In this patient circular concave rests were used on the cuspidsv Guidance in lateral excursion provided by the cuspids and premolars
- 54. Rotational Path of Insertion RPD’sv Cingulum rests prepared on the cuspidsv Positive rests prepared on the distal side of the molars
- 55. Rotational Path of Insertion RPD’sv Positive rests on the cuspids and the molarsv Lingual “I” bars used for reciprocation and encirclement of the molarsv Guidance in lateral excursion provide by the cuspids and premolars
- 56. Rotational Path of Insertion RPD’sv Cingulum rest prepared on the cuspidv Positive rest on the premolar and molars
- 57. Rotational Path of Insertion RPD’sv Guidance provided by the cuspid and lateral incisor on the left the premolar and molar on the right
- 58. Lateral Rotational Path on Insertionv Patient presents status post anterior mandibular resectionv The posterior segments of mandible are rotated to the lingual
- 59. Lateral Rotational Path on Insertionv Retention provided by the lingual surfaces of the right molars and the “I” bar on the leftv Reciprocation and encirclement for the right molar provided by the trans-occlusal rest
- 60. Lateral Rotational Path on Insertionv Trial denturev Completed RPD is inserted right to left
- 61. Lateral Rotational Path on Insertion
- 62. Lateral Rotational Path on Insertionv Surveying the cast. Note the lingual undercuts
- 63. Lateral Rotational Path on Insertionv Completed RPD with lingual retentionv Insertion path is from right to left
- 64. v Visit ffofr.org for hundreds of additional lectures on Complete Dentures, Implant Dentistry, Removable Partial Dentures, Esthetic Dentistry and Maxillofacial Prosthetics.v The lectures are free.v Our objective is to create the best and most comprehensive online programs of instruction in Prosthodontics
New Lectures
 Restoration of Posterior Quadrants and Treatment Planning
Restoration of Posterior Quadrants and Treatment Planning
John Beumer III DDS, MS
Robert Faulkner, DDS
Kumar C. Shah DDS, MS
Robert Faulkner, DDS
Kumar C. Shah DDS, MS
 Cement Retention vs Screw Retention
Cement Retention vs Screw Retention
John Beumer III DDS, MS
Robert Faulkner DDS, MS
Robert Faulkner DDS, MS
 Single Tooth Defects in Posterior Quadrants
Single Tooth Defects in Posterior Quadrants
John Beumer III DDS, MS
Robert Faulkner, DDS
Robert Faulkner, DDS
 Computer Guided Treatment Planning and Surgery
Computer Guided Treatment Planning and Surgery
John Beumer III DDS, MS
Allesandro Pozzi, DDS
Robert Faulkner DDS
Allesandro Pozzi, DDS
Robert Faulkner DDS