The vast majority of nasal defects are secondary to treatment of neoplasms. In general most partial nasal defects are reconstructed surgically whereas most total rhinectomy defects are restored prosthetically. Proper surgical preparation of the defect is and important factors in achieve acceptable cosmetic results. Osseointegrated implants have a significant impact on patient acceptance. These topics are discussed in detail in this program as well as prosthesis design, tips regarding sculpting, margin placement, and coloration of the prosthesis.
Restoration of Nasal Defects – Course Transcript
- 1. *The material in this program of instruction is protected by copyright ©. Nopart of this program of instruction may be reproduced, recorded, ortransmitted by any means, electronic,digital, photographic, mechanical, etc.or by any information storage or retrieval system, without prior permission.
- 2. This should be considered for most patients. Implant retention improvespatient acceptance and frequency of use (Chang et al, 2005)
- 3. Chang et al, 2005
- 4. Chang et al, 2005
- 5. This speeds the rehabilitation process, saves the patient asurgical procedure and provides excellent retention for thefuture nasal prosthesis.
- 6. With favorable total rhinectomy defects excellentcosmetic results such as these can be obtained andthe prosthesis will be stable well retained
- 7. Problems createda) Nasal bones affect position of the nasal tipb) Lip will always appear too short even if nasal tip of the prosthesis is shortenedc) Nasal tip will always appear too low in relation to the lipd) Nasal prosthesis will always appear too large and project anteriorly excessively because of the lip retraction and presence of the nasal bones
- 8. Prostheses fabricated for the previous patients. Thenostrils can be properly blended with the nasolabialfolds and the inferior margin is extended onto the lip.
- 9. If the defect is favorable the size and shape of the original noseshould be carefully reproduced, the nasolabial folds engagedbilaterally, and the prosthesis should be relatively symmetrical.
- 10. After recontouring the columella and tucking themargin beneath the tip of nose the appearance of theprosthesis is improved
- 11. The fabrication of an esthetic prosthesis is dependent upon the position and contours of the residual nasal structures.A good result is dependent upon the residual nasalstructures being in normal position and of normal contour
- 12. This partial rhinectomy defect is unusual because the residualportions of the nose have not been displaced and present withnormal contours. Bilateral symmetrical contours can thereforebe restored with a prosthesis.
- 13. a b
- 14. Wax sculpture is luted to the castHole is placed externally and also from the back tothrough the insure the engagement of the usablecast as shown. undercuts and proper extension onto the floor of the nose.
- 15. Polymerized silicone casting is thin, flexible and light weightStone is vibrated throughopening in back of the cast
- 16. The patient must be warned that lip margin will open uponmovement of the upper lip. Slight positive pressure in thisregion will minimize the opening somewhat.
- 17. a b c
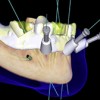
- 18. Beware of the roots of the anterior teeth.
- 19. Craniofacial implants placed in the glabella have alower success rate. If implants are planned for thissite oral lengths (7-10mm) are recommended.
- 20. Implants should not exit through the mobiletissues of the lip. Otherwise chronic tissueirritation will lead to formation of granulationtissues around the implants.
- 21. These implants are positioned too far posteriorlymaking hygiene difficult for the patient.
- 22. mpression copings are attached to the implant fixtures I ight body rubber base is applied with a syringe and L thinned with a cement spatula taking care toavoid displacing tissues of the lip and cheek. thin layer of adhesive is applied to the polymerizing A polysulfide an gauze strips are adhered to the adhesive.
- 23. Before the tissue bar is designed and fabricateda trial wax sculpting of the prosthesis must becompleted and verified on the patient.
- 24. Clip retained prostheses are preferreda) Better retentionb) Magnetic attachments tend to corrode Magnetic attachments deliver less stress to the anchoring bone and are recommended when used when only a solitary implant is available.
- 25. Best results achieved when vertical and horizontalcomponents are incorporated within the tissue bar(arrows)
- 26. a b c d
- 27. a b c
- 28. Followup period: 5 – 13 years*Conventional implants (7mm and 10mm in length) had the samesuccess rates as craniofacial implants (4mm and 5mm in length).#The two conventional length implants used have survived5 years and 7 years respectively
- 29. a b c d e
- 30. This facial prosthesis engages the maxillary obturator viamagnets in a manner shown on previous patients. Theprosthesis covers the tip of the nose and is extended laterallyon the right side of the nose.
- 31. a b
New Lectures
 Computer Guided Treatment Planning and Surgery
Computer Guided Treatment Planning and Surgery
John Beumer III DDS, MS
Allesandro Pozzi, DDS
Robert Faulkner DDS
Allesandro Pozzi, DDS
Robert Faulkner DDS
 Angled Implants
Angled Implants
John Beumer III DDS, MS
Allesandro Pozzi, DDS
Allesandro Pozzi, DDS
 Prosthodontic Procedures and Complications
Prosthodontic Procedures and Complications
John Beumer III DDS, MS
Robert Faulkner, DDS
Robert Faulkner, DDS
 Implants and RPDs
Implants and RPDs
John Beumer III DDS, MS
Ting Ling Chang DDS
Robert Faulkner DDS
Ting Ling Chang DDS
Robert Faulkner DDS